Challenges of Enhancing Effective Engagement of Community Based Organizations in Performing Provider Systems
A Discussion Paper
New York State’s Medicaid program, which funds medical care for 6.3 million residents or nearly one-third of the state’s population at a cost of more than$70 billion annually, is undergoing redesign intended to accomplish the “triple aim” of lowering costs, expanding access, and improving quality of care. The redesign effort, begun shortly after Governor Andrew Cuomo’s inauguration in 2011, is now in its seventh year and has made significant progress—per enrollee costs have been lowered, program enrollment has expanded by 1.8 million, and national quality rankings for the state have improved.1 However, much remains to be accomplished, and the Citizens Budget Commission (CBC), with support from the New York Community Trust, is seeking to help effectively implement the redesign strategies.
The redesign has four basic components. Each is proceeding in accord with state and federally approved plans, but each also confronts significant challenges. The goal of the CBC project is to examine the challenges arising in implementation and provide State officials and key stakeholders with suggestions about how implementation might be more successful. The analysis focuses on New York City and its surrounding counties, which account for more than 70 percent of statewide Medicaid enrollment and expenditures.
During 2017 and 2018 the CBC staff will prepare four policy briefs on the challenges relating to each of the four core strategies. This paper addresses the first of these implementation issues but begins with an overview of all four strategies and their challenges. Subsequent sections focus on the initial plans for the first strategy discussed, the shortfalls during the initial years, and the underlying causes of these problems; the paper ends with a set of questions and suggestions for discussion at the November 13, 2017 event with the State’s Medicaid Director, Jason Helgerson.
OVERVIEW OF STRATEGIES AND IMPLEMENTATION CHALLENGES
1. The Strategy of Creating Performing Provider Systems Faces Difficulties Integrating Community Based Organizations. Each Performing Provider System (PPS) consists of a group of providers who agree to cooperate in providing and coordinating services to Medicaid and uninsured populations in the counties in which they operate. The objective is to improve the quality of care for this population with an emphasis on reducing unnecessary inpatient and emergency room hospital care. The plan for PPSs evolved in negotiations with the federal Centers for Medicare and Medicaid Services (CMS) over a proposal for federal funding for redesign initiatives. CMS approved the project as part of its national Delivery System Reform Incentive Payment (DSRIP) program. The New York version initially provided $8.0 billion in federal funds over five years including $6.4 billion to plan and implement the PPSs; within months of initial approval $1.8 billion of combined state and federal funding was added to the support for PPSs.2
The initiative launched in 2014 with 36 applicants seeking to develop PPSs receiving planning grants.3 From this set of applicants 25 plans were approved and given the opportunity to earn five years of implementation funding beginning in April 2015. The approved PPSs include 10 serving New York City, 2 serving Long Island, and 2 serving Westchester. Each PPS has a lead organization that in most cases is a major medical center. PPSs’ sizes, structures, and compositions vary, but for each, the lead organization is responsible for ensuring that the coalition and its partners meet all PPS requirements and has fiduciary responsibility for support funds. In addition to developing a new delivery network, each PPS is responsible for executing a self-selected portfolio of up to 11 projects to engage and deliver health care to various groups of Medicaid beneficiaries.
The PPSs are intended to improve health care outcomes by better coordinating and integrating medical services from a variety of providers and by dealing better with the social determinants of health affecting Medicaid enrollees. In order to address more effectively the social determinants, PPS lead organizations were given discretion to use up to 5 percent of their funds to support services by local, nonprofit Community Based Organizations (CBOs) that do not deliver medical care or other services through the standard Medicaid program, but that have connections to local populations and can help engage them with primary care and other providers.4 However, the PPS lead organizations have had difficulties defining appropriate roles for these CBOs and developing business models for financial transactions with them. Many CBO partners who have not previously participated financially in Medicaid are concerned about how fairly they are being treated within the PPSs.
2. Health Homes Are Not Reaching All Who Could Benefit. Health Homes are organizations that coordinate care by multiple providers. Health homes are intended to serve those Medicaid enrollees with a serious mental illness or two chronic conditions, a group estimated to number about 224,000. The goal is to coordinate better the services of multiple providers involved in treating these patients, and this is accomplished by assigning the patient to a designated care coordinator. In 2012 the Department of Health (DOH) recognized 32 health homes and sent information on each eligible patient to them. It is up to the Health Home to voluntarily enroll members, and the organization receives a payment from DOH for outreach and engagement and then monthly fees for care coordination.
The Health Homes initiative was phased in during 2012. As of September 2017 only about 164,000, or just 70 percent, of the 224,000 people identified based on their multiple conditions and risk factors had been enrolled.5 A large group of people who could benefit from the program have opted not to enroll.
3. Some Patients with Extensive Care Needs are Not Being Served by Managed Care Organizations. Reliance on managed care organizations (MCOs) by a state Medicaid program is often viewed as a positive measure yielding better care and lower costs. Despite the potential benefits of MCOs, Medicaid-eligible people generally do not join them voluntarily. Few are willing to trade the possible benefits of an MCO for ability to select and use providers without restrictions set by an MCO.
New York State began a program of mandatory managed care for certain Medicaid enrollees in 1988 and subsequently expanded it in stages. By 2010 about two-thirds of all Medicaid-eligible people were enrolled in an MCO.6 The vast majority were enrolled in MCOs known as “mainstream” plans. The plans provided a range of acute care services including physician and hospital services but excluded most long-term care (nursing home, home health, and personal care) as well as treatment of behavioral health problems and some acute care services. The redesign seeks to expand reliance on managed care by broadening the range of services provided by mainstream MCOs and by increasing the types of people participating in managed care to include more aged and disabled and those with special health care needs. The eventual goal is “managed care for all.”
More than 700,000 Medicaid enrollees are “dual eligible,” that is, enrolled in Medicaid and Medicare.7 For these aged or disabled individuals Medicaid pays for the Medicare premiums and copayments and for services not covered by Medicare (most long-term care services), and Medicare pays for many acute care services. An important redesign goal is to better integrate these two programs and the care they support.
Priority has been given to two subsets of the dual eligible requiring expensive care—those requiring extensive long-term care and the developmentally disabled. Beginning in 2012 dual eligible people requiring extensive long-term care have been required to enroll in long-term managed care plans covering long-term care benefits but not necessarily covering acute care benefits. As of October 2017 about 198,000 people had enrolled in a managed long-term care program.8 In order to integrate long-term care and acute care services for this population, the State gained approval in 2013 from CMS to launch a Fully Integrated Duals Advantage (FIDA) program that offers one managed care entity to provide both types of services. However, enrollment is not mandatory, and few people have enrolled. As of October 2017 only about 4,500 people were enrolled, compared to initial projections of as many as 100,000.9
Designing a managed care program for the developmentally disabled required extensive discussions with CMS and eventually yielded a federally approved initiative for the Fully Integrated Duals Advantage for Individuals with Intellectual and Developmental Disabilities (FIDA-IDD) program. The plan has a more narrowly defined target population: of the approximately 50,000 developmentally disabled individuals with multiple chronic conditions statewide, approximately 10,000 who are eligible for FIDA-IDD live in the service area of New York City, Long Island, and the counties of Rockland and Westchester.10 The FIDA-IDD plan opened enrollment on April 1, 2016 and is administered by the Partners Health Plan. All enrollment is voluntary, and it remains to be seen how effectively it will operate.
4. Shifting to Value-Based Payments is a Complex Process. The most recent redesign strategy was developed as part of the agreement for the federal DSRIP program. The goal is to shift from payments to providers based on the volume of services (for example, number of physician visits or hospital admissions) to the quality of care provided as reflected in outcomes (for example, number of patients treated appropriately for diabetes during a year). Since a goal is to have most Medicaid enrollees in an MCO paid with a monthly capitation payment, the value-based strategy applies to payments by MCOs to their participating providers.
Planning for conversion to value-based payments (VBP) began in 2014. The plan recognizes multiple forms of value-based payments distinguished by the scope of services covered and the nature of risks the providers assume. The timeline for implementing value-based payments requires use of such payments to begin in the third year of the DSRIP program (April 1, 2017 to March 31, 2018) and in the final year at least 80 percent of payments must use a value-based approach with at least 35 percent involving significant risk sharing.11
The VBP strategy faces difficult technical and policy choices. Suitable quality of care and health outcome measures must be identified and collected, and weights assigned to the quality dimensions of payments. The application of this approach to a comprehensive set of services for diverse populations is a complex task which stakeholders and DOH staff are pursuing, but much work remains to be done before the scheduled start of implementation in fiscal year 2019.
INITIAL PLANS FOR CBO ENGAGEMENT IN THE PPSs
As previously noted, PPSs are being developed as part of a demonstration program supported by $8.2 billion from the federal and state governments under a program known as DSRIP. Under DSRIP 10 states including New York have been given federal funds to improve the health care delivery systems for low-income populations. New York’s initiative is unique in its call for PPSs as a mechanism for achieving these improvements, notably a decline in unnecessary hospitalizations and emergency room use and improvements in health care outcomes for the indigent.
New York’s DSRIP program spans six years from April 2014 to March 2020. The first year was devoted to planning, and the next five years are for implementation.12 The plans included a selection of between 5 and 11 projects from a menu of 44 projects, with a minimum of at least 2 projects related to system transformation, at least 2 projects related to clinical improvement, and at least 1 population-wide project.13 Financial support during the implementation years is contingent on meeting reporting requirements, process milestones, and performance goals included in the initial plan, with the share of payments dependent on performance goals increasing in each year.
Statewide the initiative established 25 PPSs.14 The 14 PPSs in the New York City region and their funding allocation and assigned populations are identified in Table 1.15 Funding was based largely on the size of the assigned population, which is the number of Medicaid and uninsured people the PPS seeks to serve.
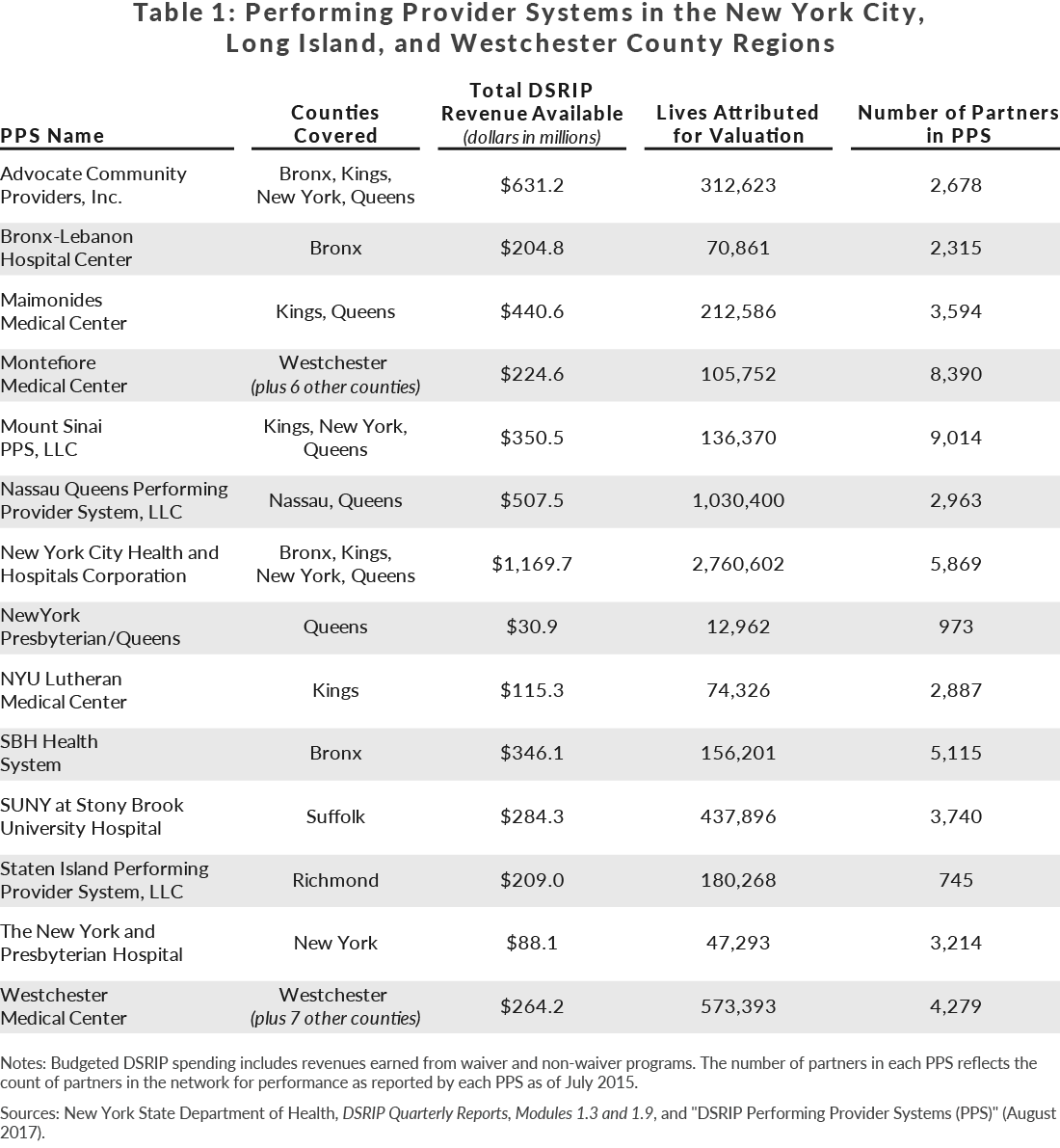
The PPSs are not necessarily formal legal entities; they typically are voluntary collaborations among multiple entities that agreed during the planning process to cooperate in improving health care delivery. Each PPS has a “lead organization” which has fiduciary responsibilities for the funding it receives semiannually from DOH, and which provides leadership for the coalition. Statewide 23 of the 25 lead organizations are major medical centers; among the 14 PPSs in the New York City region, 13 have major medical centers as a lead organization, and 1 has a medical group academically partnered with a medical center as its lead organization. The number of entities committing to each PPS is large with many being primary care physicians and behavioral health and other providers with practices in the region served by the PPS. Providers can be a participant in more than one PPS.
Each PPS was required to establish a governance structure to set policy and guide implementation. The governance section of the PPS application included this requirement: “The PPS must include a detailed description of how the PPS will be governed and how the PPS system will progressively advance from a group of affiliated providers to a high performing integrated delivery system, including contracts with community based organizations.” The PPSs varied in their proposed governance structures, but typically established an Executive Committee with subcommittees. The Executive Committees vary widely in size and composition with some not including representatives of CBOs, others including one CBO member selected by the lead organization, and others having numerous CBO members drawn from organizations participating in the planning process. Governance plans also typically include a Project Advisory Committee with an advisory role to the Executive Committee, and these committees are typically large with representatives from all stakeholder groups including CBOs.
Each PPS plan indicates the number of CBOs committed to participating in the planned activities and the amount of allocated funding the CBOs would be eligible to receive. CBO commitments were detailed for each of the projects selected in the PPS plan. Table 2 shows for the 14 New York City region PPSs the amounts budgeted for CBOs during the five-year implementation period and that allocation as a share of total funding. Among 12 of the 14 PPSs less than 5 percent of the funds were allocated to CBOs; one allotted 7.3 percent and another 12.9 percent.
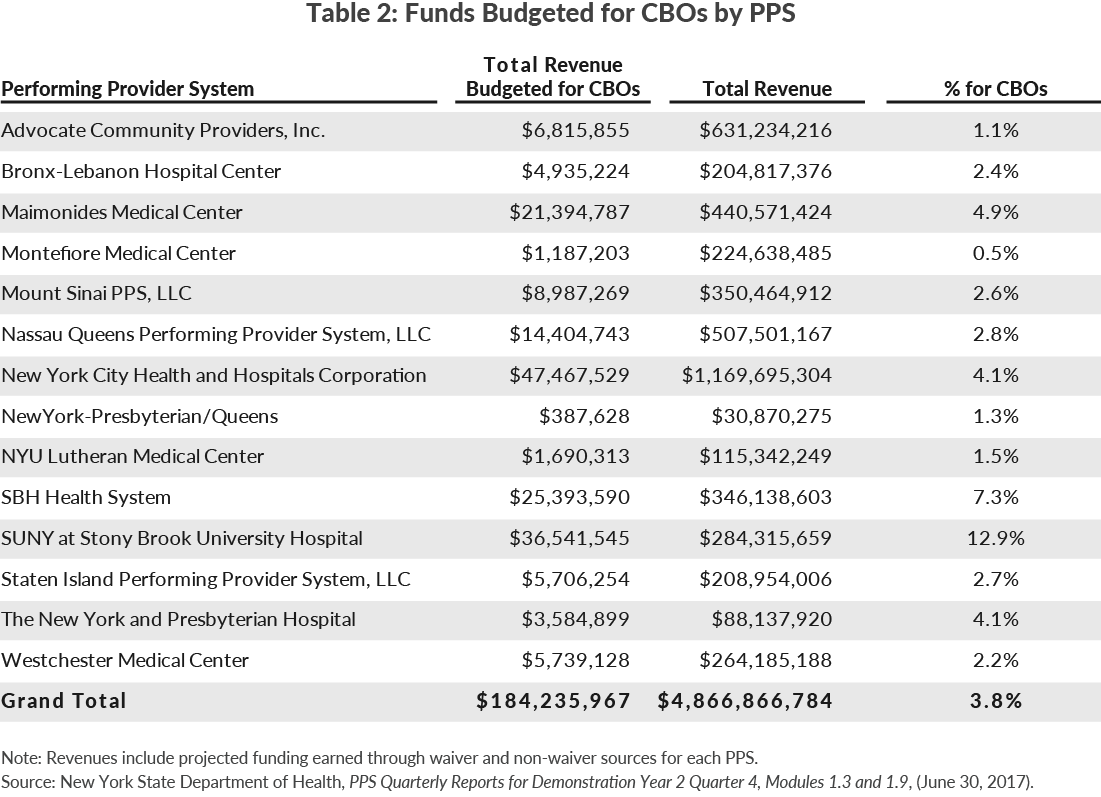
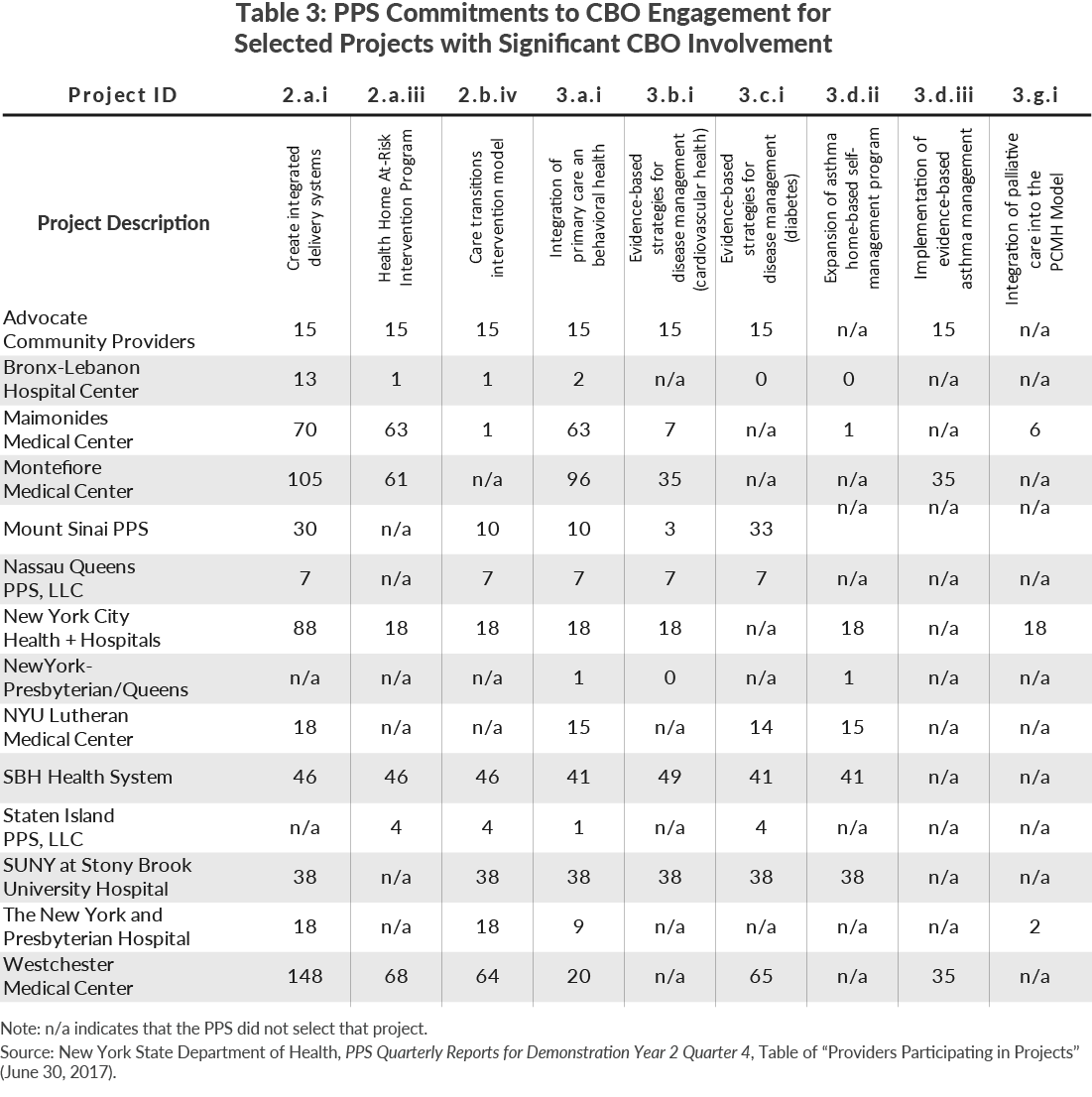
Table 3 shows for each PPS the number of CBOs committed to each of nine projects most frequently selected by the PPSs and for which CBO engagement was most relevant. (Many of the projects related to clinical improvement did not necessarily involve CBOs.)
During the planning and early implementation stages, the State guidelines for the definition of a CBO was linked to the federal requirement that no more than 5 percent of the funding go to organizations that were not participating in the Medicaid program.16 The PPSs were asked in planning materials and in initial implementation reporting documents to identify as CBOs only those local nonprofit partners that did not have a Medicaid program identification number, which is necessary for financial participation in the program. Many nonprofit organizations consider this a highly restrictive definition, because numerous organizations with strong community ties participate in the Medicaid program as providers of a range of services including outreach and coordination of care, as well as behavioral health and other medical services. However, state planning and reporting documents specified the narrower definition of CBOs and classified the other entities receiving Medicaid funding in other categories such as clinics and Health Homes.
In late 2015 as part of its planning for implementation of VBP the State revised its approach to defining a CBO. The approach recognizes three “tiers” of CBOs: (1) those in the initial definition, (2) organizations providing nonmedical services but which had Medicaid provider numbers and received some Medicaid payment for services such as transportation or other supports, and (3) certain organizations with Medicaid provider numbers that provided clinical as well as support services to special populations such as those with developmental disabilities and behavioral health problems.17 Beginning in 2016 reporting requirements were adjusted to include the variety of organizations, but separate data was also reported for the previous “Tier 1” category.
The data in the planning documents suggest three important characteristics of the planned Tier 1 CBO engagement in PPSs. First, the lead organizations varied widely in the extent to which they anticipated such CBO engagement. At the low end of the spectrum, New York-Presbyterian Hospital Queens identified only one CBO with which it would work, Staten Island four, and Nassau Queens seven. At the other end, Westchester identified 148 CBOs for one of its projects, Montefiore identified 105, and New York H+H identified 88.
Second, CBO engagement was concentrated in a few projects and focused on certain types of activities. These include outreach to certain target populations, assistance to providers in coordinating care particularly for patients with behavioral health issues, and training in cultural competence for provider staff.
Third, the average amounts budgeted for each CBO were relatively small. While averages may be misleading because the total funds were not necessarily intended to be spread evenly, the indicator is still revealing of the modest amounts involved. With the exceptions of Nassau Queens and Staten Island, the per-CBO five-year amounts calculated from the data in Tables 2 and 3 are all less than $962,000 and as little as $3,000, suggesting annual amounts ranging from under $200,000 to under $1,000. The relatively higher amount of funding per CBO within the Nassau Queens and Staten Island PPSs is a product of the commitments by those PPSs to engage few CBOs, not a product of an unusually large fiscal commitment.
THE PACE OF IMPLEMENTATION
Initial plans for Tier 1 CBO engagement involved varying degrees of participation in governance and limited, but also varying, commitments of financial support. Implementation of each type of engagement proved to be slow during the initial DSRIP period.
During the planning period the lead organizations varied widely in the extent to which they sought and received input from CBOs. All were aware that DOH was seeking some degree of CBO engagement in the PPSs to be proposed. Some lead organizations had limited pre-existing ties to CBOs and pursued their planning with limited outreach to new entities. Other lead organizations had some working relationships with CBOs and sought their participation, and some extended outreach to identify new potential partners. In other cases CBOs were aware of the PPS initiative and sought to develop new relationships with the lead organizations.
Some initial tension arose during the planning period because CBOs were aware that the lead organizations had received financial support to conduct the planning—a collective total of $70 million statewide—but the lead organizations made little or no funding available to CBOs who participated in the planning process.18 CBO leaders felt they were asked to commit staff time “on spec” with the hope the relationship might lead to future contracts. In some cases CBOs committed significant senior staff time to the planning process with no financial support from the lead organization. From the lead organizations’ vantage, CBOs were treated the same financially as other external organizations involved in planning, and in some cases the lead organizations had to draw upon internal resources as well as the DSRIP funds to meet the extensive planning requirements.
Limited financial support to CBOs continued in the first two years of the PPSs. Table 4 presents the amounts disbursed by each PPS to Tier 1 CBOs during the first two years (April 2015 to March 2017). The total of $11.8 million is about 6 percent of the five-year budgeted total shown in Table 2. The low rate of payments to CBOs in the first two years is striking in light of the planned activities, which often related to early outreach in the projects and training in cultural competence for the staff.
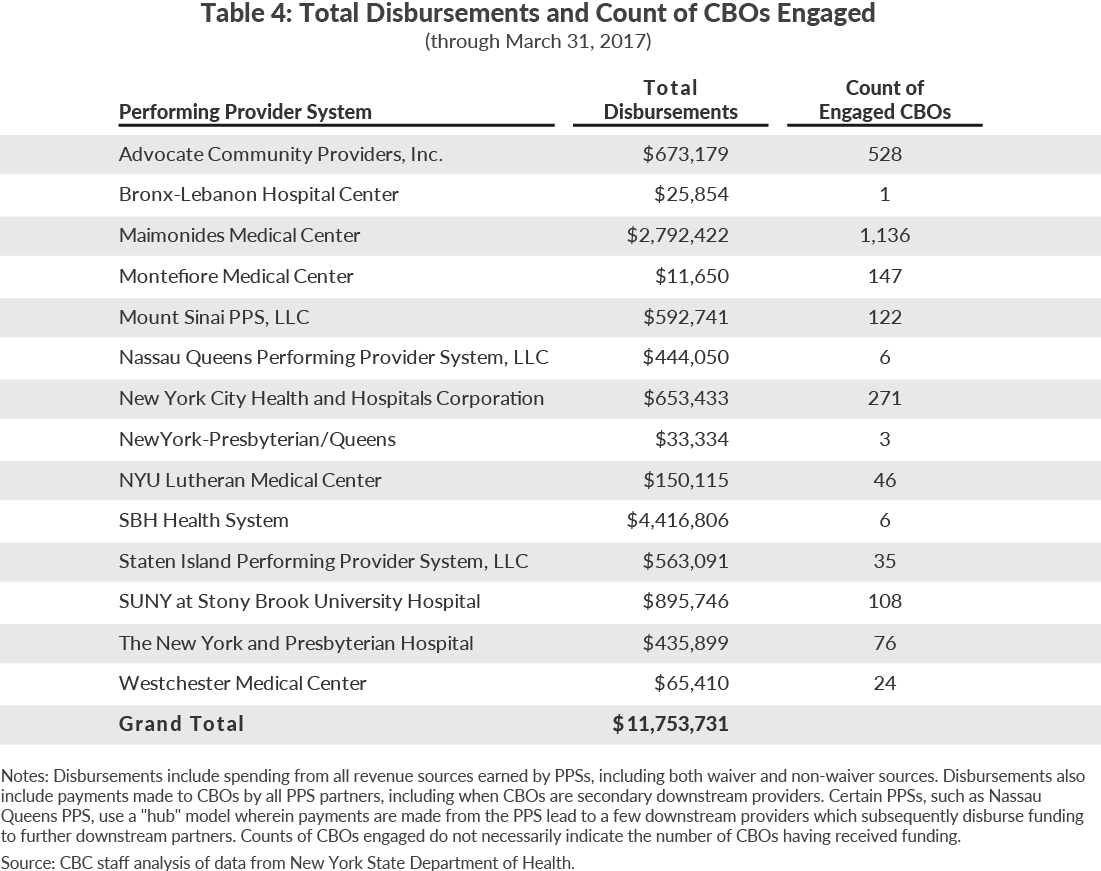
Among the 14 PPSs, four had payments less than $100,000, and eight had payments between $100,000 and $900,000. Only two PPSs had payments over $1 million.
The bulk of the funding went to relatively few organizations. Information on specific recipients is available for $7.4 million of the $11.8 million in payments.19 The single largest recipient is Local 1199 of the Service Employees International Union, which received more than $2.3 million from the PPSs led by Maimonides and SBH Health System; the union qualified as a CBO under the initial definition, and it is performing staff training. This payment accounts for nearly one-quarter of the total payments and more than half of Maimonides’ payments to Tier 1 CBOs.
The only other organization to receive more than $1 million is a.i.r. nyc, which focuses on helping those with asthma. It received nearly $1.5 million from three PPSs for work on the asthma-specific projects they selected. Together this and the Local 1199 payments account for more than one-third of the subtotal for which information was reported.
Seven additional CBOs received payments of more than $100,000, with the largest reaching just over $600,000. Together this group received about $2.2 million. These transactions included payments from the SBH Health System PPS to the Bronx Regional Health Information Organization (RHIO), payments from New York City H+H to the municipal Department for the Aging, payments from the Staten Island PPS to two CBOs, a payment from the Stony Brook PPS to Brentwood Pediatric and Adolescent Associates, payments from three PPSs to Arthur Ashe Institute, and payments from two PPSs to Health People, Inc.20 These seven entities and the previously identified two organizations account for more than three-quarters of the total payments on which information is available.
While relatively few Tier 1 CBOs account for much of the money paid to these types of CBOs, Table 4 also indicates that a larger number of CBOs are “engaged” with the PPSs. The reporting of “engaged” CBOs is part of the PPS periodic reporting, but its meaning is not financial. Engagement does not require receiving money; rather it indicates an agreement has been reached for participation in some activity for which payment may or may not be planned. Engagement is also reported for separate projects, so one CBO maybe counted as engaged multiple times if it participates in more than one project. Thus for some PPSs the “engaged” count in Table 4 reflects the counting of some CBOs more than once. Nonetheless, these reported figures suggest the PPSs are seeking to relate to a wider range of CBOs than those Tier 1 organizations to which they are making payments.
In light of the limited CBO contracting activity, DOH sought to provide assistance in the process. A preliminary analysis suggested a key stumbling block was a lack of technical capacity in the contracting process among smaller CBOs with limited administrative staff and financing that was primarily philanthropic rather than governmental or more grant than contract based. In May 2016 the State issued a Request for Applications (RFA) to award $7.5 million to CBO planning consortiums across the State. These consortiums would bring together small CBOs, defined as those with annual budgets of $5 million or less.21
The consortiums are each led by one eligible CBO and organized geographically, with $2.5 million available for each consortium covering New York City, the suburbs of Long Island and the Mid-Hudson, and the rest of the State. In December 2016 one-year awards of $2.5 million each were made to the Arthur Ashe Institute and the S2AY Rural Health Network, Inc. in the New York City and Rest of State regions, respectively. The RFA for Long Island/Mid-Hudson was re-issued, and awarded in August 2017 to The Health and Welfare Council of Long Island. In each case consortium activity began a few months after the award, so the initiatives are still under way.
The CBO Planning Grants included important requirements to limit participation to small organizations that had at least three years of experience working in their communities. The grants will allow the consortium to work with other eligible CBOs in the region, and the consortium is required to hire an external consultant to help the CBOs develop the infrastructure and planning necessary to participate in DSRIP. The grant is intended not only to provide funding and support to CBOs in the context of DSRIP, but also to “further explore a financially sustainable infrastructure to meet ongoing and longer term engagement in system transformation.”
Another DOH initiative that helps promote CBO involvement in health networks is part of the effort to promote VBP. VBP is seen as a long-term solution for continuing to transform health care delivery through financial incentives after the conclusion of the DSRIP waiver. VBP arrangements shift insurers and MCOs in the State from paying for volume of services, and instead pay providers for improving quality of health care. The State’s plan for expansion of VBP, known as a Roadmap, sets forth a schedule for conversion to this type of payment by the Medicaid program’s MCOs. The Roadmap requires certain VBP arrangements to include one or more Tier 1 CBOs. These arrangements require payments from the MCO directly to the CBO or indirectly to the CBO as a subcontractor to a medical care provider such as a hospital, but do not require the CBOs to take on any financial risk.
Some PPSs have elected to support CBOs in contracting and VBP integration through designating some available resources as “Innovation Funds.” PPSs use the Innovation Funds to support partners for creative problem solving related to social determinants of health. PPSs are using Innovation Funds to support projects such as nutrition training, to support CBOs in VBP planning, and for other short-term projects to help small CBOs become—and remain—effectively engaged in achieving DSRIP and VBP goals.22
Participation in VBP arrangements is a major opportunity for CBOs to engage in improving health care delivery networks on a financially viable basis. However, these relationships are dependent on funding from MCOs rather than from PPS lead organizations. The new opportunity is an additional avenue for engagement, but does not necessarily expand or accelerate relationships with PPSs, and could be an alternative that shifts attention from the PPS relationships. In addition, the minimum requirement of each MCO having direct or indirect ties to just one Tier 1 CBO is viewed by many of these organizations as a low bar; the hospitals that contract with MCOs typically already have some modest relationship with at least one Tier 1 CBO, meaning the new mandate likely will require little or no change from existing arrangements.
A clear understanding of any obstacles to effective engagement has been made more difficult by two features of early DSRIP implementation. First, many parties tend to define engagement as equal to cash flows rather than defined more broadly to encompass a range of arrangements. Money is certainly important and often necessary for effective engagement, but other effective arrangements are possible and can be common. Participation through referrals, outreach, and coordination of services, as well as other mechanisms, should be recognized as part of effective engagement.
Second, the scope of CBOs with which effective engagement is being promoted and assigned priority has been narrowed by the conflation of the federal 5-percent limit applied to non-Medicaid provider funding and the approach to defining CBOs. The more recent tiered definition of CBOs corrects and refines the initial limited definition, but the deeper and more effective engagement of Tier 2 and Tier 3 CBOs has not been elevated as a concern to the level of attention to Tier 1 CBO engagement. More uniform concern with the full range of CBOs could contribute to broader actions achieving effective engagement.
Once these potentially confusing aspects of the issue are taken into account, it is possible to more clearly identify the more substantive obstacles to effective engagement. Based on CBC staff interviews with multiple stakeholders, four issues appear to undermine New York’s progress toward effective engagement of CBOs:
- Limited evidence for selecting appropriate roles for CBOs in addressing health delivery needs;
- Difficulties designing suitable business models for contracting for non-clinical services from CBOs;
- Uncertainty about the future governance and sustainability of PPS entities; and
- Leadership skepticism among some CBOs and some lead organizations.
Limited Evidence for Selecting Appropriate CBO Roles
As noted earlier, initial plans for CBO involvement tended to focus on their role in outreach to difficult to serve populations and their contribution to enhancing hospital staff cultural competence. These are typically “up front” activities that help make medical services more accessible and effective, but these activities are less directly involved in addressing the social determinants of health. As PPSs seek to address social determinants they encounter less certainty about the effective roles of CBOs.
Two concerns arise in seeking CBO relationships that deal with social determinants. First, limited systematic evidence is available about the cost-effectiveness of such programs. Housing support, employment assistance, transportation services, nutrition advice, and other wellness coaching all have not only an intuitive appeal and some successful documented examples, but more systematic evaluations of pilot programs and refined efforts at identifying subpopulations most susceptible to such interventions are rare. In addition, the assessments calculating return on investment do not always distinguish between overall societal savings and specific health provider bottom lines. Thus it is difficult for lead organizations to select with confidence roles for CBOs that are relevant to these types of initiatives. DOH has responded to this concern by providing resource material that describes and documents results of interventions relating to the social determinants of health including estimates of cost-benefit ratios for some programs.23 Such materials are helpful and provide guidance, but some PPS leaders are not certain the examples are appropriate for their circumstances or are rigorous enough in their evaluations.
Second, the time frame for effective interventions affecting social determinants likely is longer than that for the DSRIP waiver. PPSs are under pressure to produce measurable results in less than five years, but the impacts of many support services on health status may not be evident until even longer times have elapsed. Thus lead organizations have limited incentives to try to put in place these types of relationships with CBOs. DOH’s resource material includes examples of programs that have produced positive results in less than five years, although this material is from national sources and from studies that sometimes rely on indicators of health status that are not necessarily indicators of health expenditures.
Designing Business Models
When CBOs and lead organizations reach an agreement on a desired relationship, it is often difficult to design a financial contract to accommodate that role. The two entities approach contacting from different frameworks. Hospitals and other medical providers have relationships with payers that are based on payment for specific services rendered with payment on a per service basis. CBOs often derive a significant share of their funding from philanthropy, which is typically awarded without specific service performance requirements, and/or from government contracts awarded annually on the basis of budgeted amounts that are derived from staffing requirements and not necessarily attached to specific service volumes. The different frameworks make it difficult to reach agreement on a basis for payments from lead organizations to CBOs.
Moreover, even as CBOs accept a different contracting framework, the nature of the services being procured can make it difficult to adapt the medical services model. That is, units of service for certain preventive or support activities may be hard to define and assign unit costs. For example, what can be the basis of payment for CBO efforts to prevent alcohol or drug abuse among youth? Services which more readily lend themselves to unit of service payments, such as enrollment in staff training programs and completion of resident surveys, have often been the basis for the limited contractual payments made by lead organizations to CBOs.
Future Uncertainty
New York’s DSRIP initiative creates PPSs as entities intended to be sustainable beyond the five-year waiver period. CBOs are intended to be long-term partners in these viable networks and typically to participate in the governance of the entities created.
This longer-term vision is proving difficult to realize because of uncertainty about the viability of the PPSs as ongoing collaborations.24 This uncertainty is related to two types of financial risk. First, a significant portion of the federal DSRIP money is conditioned on performance in the later years, and some lead organizations are concerned they may not qualify for the full payments. In this case, not all budgeted plans may be realized. The concern about future revenue also has led some PPS managers to slow actual expenditures relative to their initial budgets in order to build reserves to cover any shortfalls in revenue in the later years. This cautious financial management may be a factor in the slow pace of contracting for CBO services. Through March 31, 2017 PPSs have earned nearly every dollar available to them for meeting metrics, but most of those metrics were reporting activities. The shift toward payments based on performance increases year after year. In the final two years 64 percent and 82 percent, respectively, of payments will be based on performance. (See Table 5.)

The second financial risk relates to viability after the initial five-year period. Current plans have the PPSs federal revenue dropping from a collective total of nearly $1 billion in the final year to zero thereafter. While DSRIP waivers in some states have been extended beyond the initial period, this is not a strong possibility for New York given the changing policies of a new federal administration. Some lead organizations and CBOs believe that PPSs many not have a lifetime extending after 2020 and are not inclined to invest time and energy to develop new relationships in the absence of longer-run, positive fiscal prospects.
Future financial uncertainty is also related to a shift in DOH’s approach to PPSs’ role in the transition to VBP. Initially VBP was a part of the DSRIP program and incorporated PPSs as a mechanism for such payments. The evolution of the VBP strategy has shifted to relying primarily on MCOs as the mechanism for VBP. Post-DSRIP, some PPSs may continue as entities contracting with MCOs, but another important aspect of CBO engagement will be links between CBOs and MCOs that may not include ties to a PPS.
Leadership Skepticism
Trust is an important element in developing constructive relationships. Unfortunately some principals among some CBOs and lead organizations approach the development of PPS networks with skepticism about the others’ commitment to and capacity for effective relationships.
Among CBOs, the most extreme viewpoint held by a few is that DSRIP is simply a device created by State and federal officials to channel additional federal funding to the hospitals in exchange for their cooperation in other cost containment initiatives. From this vantage the requirement for CBO engagement is little more than a “front” to help justify the added hospital subsidy. This cynicism may have its origins in past experiences and impressions, but is seen as recently justified by the uncompensated efforts of CBOs in the planning process and the slow pace of CBO contract development and payments.
Less cynical CBO leaders are nonetheless skeptical about the lead organizations’ commitment to CBO engagement on other grounds. They recognize PPS development is a complex process and that other partners, notably primary care physicians and behavioral health providers, are perceived as more important in the initial stages by hospital leaders and therefore draw more attention and priority than do CBOs. At best, they see themselves as a secondary concern for lead organizations’ leadership, and as such, given lower priority than other challenges involved in PPS development.
Among those at the lead organizations, multiple reasons are given for the caution and slow pace of developing CBO relationships. The limited administrative capacity at smaller organizations raised concerns about fiscal accountability; this is being addressed by the State-supported coalition technical assistance, but the need for this support justified for some the initial caution and skepticism about CBO managerial competence. In addition some lead agency staff were surprised in the planning process by the large number of relatively small CBOs in their geographical areas and became concerned that dealing with numerous small agencies to reach multiple fragmented target populations might be more time consuming and difficult than the potential benefits justified.
DISCUSSION QUESTIONS
The purpose of this paper is to identify possible ways to enhance effective engagement of CBOs with PPSs and, for the longer term, with other evolving health delivery structures. As with medical treatment, the identification of appropriate interventions relies on an accurate diagnosis of the problems. Accordingly, a good starting point for discussion is whether the issues identified in this paper are the most important challenges. Specifically:
- Are the four issues identified the most important ones?
- Have other important challenges been overlooked, and, if so, what are they?
If the identified issues are critical to future progress, then potential strategies for improvement can be considered. For purposes of discussion, CBC staff presents three such initiatives: (1) intensified State action to promote adoption of arrangements with CBOs that have demonstrated some success in specific arenas and can feasibly be replicated; (2) mutual acceptance among CBOs and lead organizations of modest expectations for financial arrangements related to arenas in which clear and effective roles for CBOs are not readily apparent and experimentation is needed; and (3) early and explicit attention to planning future arrangements for effective CBO engagement after the DSRIP waiver terminates.
Intensified State action to promote replication of effective arrangements
DOH, as previously noted, has prepared resource materials identifying examples of CBO engagement that have evidence of positive returns on investment, including some with gains within a five-year time frame. Further development of these examples and clear descriptions of how they help in the specific projects which PPSs have selected might provide a basis for more aggressive promotion of such arrangements.
A potential resource for intensified efforts is discretionary funding in the DSRIP waiver. The State may be able to use unexpended funds and funds allocated but not earned by some PPSs as a pool for supporting replication of successful initiatives. Such available funding should be identified early, and its availability made known.
- How numerous and convincing are these models for replication?
- What are the pros and cons of intensified State action to promote particular types of CBO contracts?
- What are the best tools for State action – technical assistance, incentives, sanctions, or others?
Mutual acceptance of more modest expectations
Many potential forms of CBO engagement cannot be based on firm evidence of past success. Both parties should recognize that significant risk is involved. Lead organizations should not expect virtual assurance of large health outcome improvements from modest investments, and CBO leaders should not expect substantial financial investments without prior demonstration of positive performance. In many instances of planned CBO engagement, both parties should be more modest in their initial expectations of each other and allow time for more trusting relationships to develop based on actual experience.
- What should be a reasonable scale of investment in risk laden initial arrangements?
- What standards of performance in advance of contractual relations are reasonable expectations for lead organizations?
Early and explicit post-DSRIP planning
The DSRIP project is beginning the last half of its implementation period. Given the previous pace of CBO engagement, much of the planned activity will have to take place in this late stage. But lead organizations and CBOs recognize this is a difficult process absorbing valuable and scarce leadership time and attention. Some question whether to make the necessary investment given the uncertainty over the future of PPSs as organizations.
In order to provide these stakeholders with a clear basis for planning their relationships, the State and CMS should more explicitly address the options for the future of PPSs. Potential post-2020 funding should be identified and expectations about sustainability set forth.
Strategic attention should also be given to identifying future funding streams for CBO participation in health care delivery. If such engagement is to become wider and more effective, then it will require a reliable funding base after the current DSRIP program ends. Given the present federal policy environment, extended waiver funding and new federal funding streams are not strong possibilities. While cost containment pressures on current Medicaid benefits will persist, Medicaid payments could support effective—and long-term cost saving—CBO activities. This is already the case for some Tier 2 and Tier 3 CBOs receiving direct payments, and greater use of such services is possible. The mandated payments to Tier 1 CBOs through VBP arrangements with MCOs (and non-mandated but effective arrangements with other CBOs) can also make available Medicaid funds to CBOs, although MCO premiums may have to be adjusted to support this.
Perhaps the most fiscally viable strategy to support broader effective engagement is better coordination with the current categorical, non-Medicaid funding streams supporting Tier 1 and other CBOs. The CBOs have federal, state, and local programs which separately support their activities, and better coordination of this funding with available Medicaid funding could make arrangements more cost-effective. Categorical programs for the population involved in the criminal justice and juvenile justice systems reportedly have been used in this manner in Los Angeles, and this arena could be a priority for future action in the New York City region.
- How feasible is such planning at this point?
- How likely is the sustainability of current PPS organizations, and what are the alternative organizational arrangements that might be viable?
- What is the most desirable future vision of CBO effective engagement in health care delivery – via PPSs, MCOs, direct support from State agencies, or other options?
- Should the population involved with the criminal and juvenile justice systems be a priority for future CBO engagement?
APPENDIX: LIMITED LESSONS FROM OTHER DEMONSTRATIONS
New York’s effort to develop PPSs is taking place under one of 10 federal DSRIP demonstration programs and four “DSRIP-like” programs. While these programs share some common goals in improving health care delivery to low income populations, they vary in their scale and focus. Most of the projects are of a smaller scale than New York’s, and greater engagement of CBOs is not a key element in their reform efforts.
Six of the national DSRIP initiatives were approved before New York’s program and potentially provide some lessons. However, two of the state programs, Kansas and New Mexico, are of limited scale and do not include significant emphasis on inclusion of CBOs. The New Jersey program has a five-year span with $292 million in federal funds available to 63 hospitals in the state. It is not a target of this analysis because the hospitals’ projects focus on eight specific chronic diseases and did not require participation of CBOs (although some may have done so).
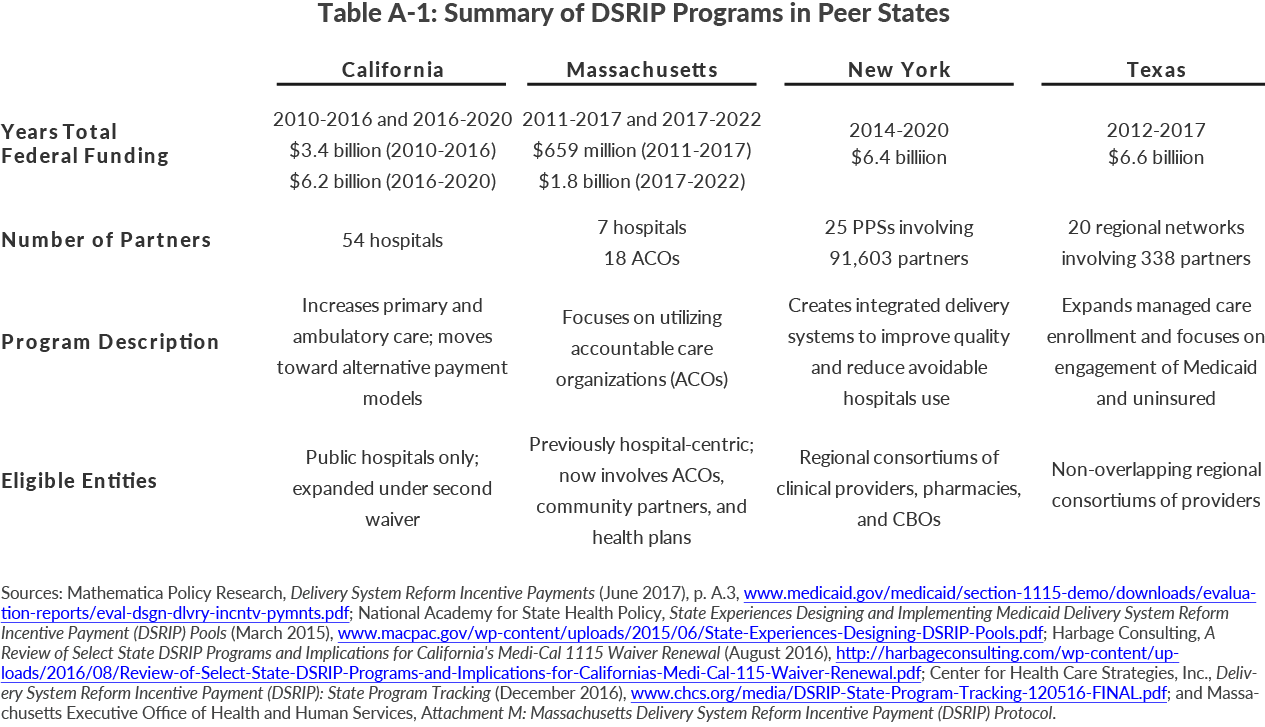
The potentially more relevant projects are those in California, Texas, and Massachusetts. (See Table A-1.) The California project was the first approved; it began in 2010 and was extended in 2016 to 2020 with total funding over the entire period of more than $9.5 billion. The Texas project was approved in 2012 and is scheduled to end in September 2017 with funding of nearly $6.7 billion. The Massachusetts project was approved in 2011 and renewed in 2017 to June 2022 with total funding of more than $2.4 billion.
The California program was initially established as a way for the state to continue to receive special supplemental Medicaid payments after the implementation of the Affordable Care Act (ACA) and targeted funding to the state’s public hospitals, which were receiving these ACA funds and faced future cuts. Participants in the program were 17 public hospitals, including 12 county-owned facilities and 5 University of California hospitals. Payments were conditioned on the hospitals implementing specific projects in each of four categories: (1) ambulatory care infrastructure development, (2) redesign of care delivery, (3) tracking of population health measures, and (4) improving urgent care. Ten hospitals later added projects in a fifth category, improving quality of care for patients with HIV.
An evaluation of the California program using self-reported data from the hospitals found that the vast majority of the projects were implemented and yielded improvements in quality of care. Other findings relevant to the New York effort were that projects selected for the program were often continuations or expansions of ongoing initiatives at the hospitals and were more often credited with having their greatest impact on quality improvement (56 percent of projects) versus improving patient outcomes (36 percent) or increasing cost containment/efficiency (9 percent).25
A 2015 Kaiser Foundation review of DSRIP programs in four states including California observed this about the California program: “Unlike more recent DSRIP initiatives, it does not require these public hospitals to establish new partnerships with community clinics or social service agencies, but, the state’s public hospitals already have relatively extensive relationships with such entities and, in some instances, even operate their own Medicaid managed care plans.”26
The Texas DSRIP program was approved in 2012 and in some ways more closely models the New York program. The Texas program is organized into 20 Regional Health Care Partnerships (RHP) covering the state. Each RHP has an anchor organization which is the single point of contact with state and federal agencies; the anchor is typically a public hospital or the public agency (such as a county health department) in the region. The anchor is responsible for developing a needs assessment and plan for the region and for identifying projects to be undertaken by providers in the region in order to qualify for federal funding. The projects must be distributed among four categories: (1) infrastructure development, (2) program innovation and redesign, (3) quality improvements, and (4) population-focused improvements.
The 20 RHPs include 309 distinct Medicaid provider organizations, and these individual organizations are responsible for implementing the selected projects and receive payments based on successful implementation of the projects. Each RHP was required to have a minimum number of projects from each category, but providers proposed notably more than the minimum, so 1,491 distinct projects were launched under the program.27 Although the organizations implementing the projects are Medicaid providers rather than non-Medicaid CBO entities, some of the projects may involve using services of such CBOs. No detailed analysis of the participants in the multiple projects is available, but it is likely that some CBOs are involved because many projects relate to improving services to those with behavioral health issues and improving population based health metrics. However, no evaluation addressing the extent to which these types of initiatives have been successfully implemented is readily available.
Massachusetts created its program, the Delivery System Transformation Initiative (DSTI) program in 2011 with nearly $700 million in funding. It consisted of seven hospital-led efforts to reform delivery of care.28 The hospitals initiated individual projects to address each of the four areas: (1) development of an integrated delivery system built on Patient-Centered Medical Home principles; (2) implementation of innovative care models to improve quality of care and health outcomes; (3) development of capabilities necessary to implement alternative payment models; and (4) outcomes and improvement measures related to Category 1-3 projects and population-focused health outcome improvements. During this initial five-year phase relatively little emphasis was given to relations between the hospitals and community-based organizations.
The currently renewed Massachusetts DSRIP waiver is allocated $1.8 billion of federal funding from 2017 to 2022. Massachusetts will invest $1.1 billion of the total in accountable care organizations (ACOs).29 ACOs are groups of providers responsible for caring for a patient’s full medical needs with the goal of improving care by keeping patients in the most appropriate care settings, such as through receiving home- and community-based care to avoid hospitalizations.
Massachusetts will spend an additional $546 million in the Community Partners Program. This initiative will invest in behavioral and long-term care service providers and in approved community service agencies (CSAs). CSAs are community-based organizations facilitating intensive care coordination for certain enrollees. CSAs are already approved under the State’s general Medicaid State Plan. As part of the new DSRIP initiative, the 32 CSAs will provide additional care management support for enrollees with the most complex health care needs.30 The Community Partners and CSAs may contract with CBOs as part of the enhancement of their care management work with high utilizers.31 This initiative is similar to New York’s PPS initiative, which preceded it, in focusing on high-utilizing enrollees and facilitating coordination between community organizations—both clinical providers and social organizations—to improve individual and population health, but its recent launch means there is little evidence to date on how successfully it is being implemented.
Footnotes
- See: Charles Brecher and Mina Addo, What Ails Medicaid in New York: And Does the Medicaid Redesign Team Have a Cure? (Citizens Budget Commission, May 2016), https://cbcny.org/research/what-ails-medicaid-new-york.
- Following the finalization of projected DSRIP valuations in May 2015 the State created additional programs in order to increase the funding available for projects at certain PPSs. The primary beneficiaries of the State-created non-waiver programs were nonpublic PPSs in the downstate regions. These programs–the Equity Infrastructure Program, Equity Performance Program, and Additional High Performance Program–provided $1.8 billion in addition state and federal funding by repurposing funding previously budgeted by the State for DSRIP support efforts. These revenues are referred to in PPS quarterly reports and throughout this report as “non-waiver revenue.” See: New York State Department of Health, Supplemental DSRIP Programs (October 2015), www.health.ny.gov/health_care/medicaid/redesign/dsrip/vbp_initiatives/docs/equity_programs_and_ahpp.pdf, and “Supplemental DSRIP Programs” (October 2017), www.health.ny.gov/health_care/medicaid/redesign/dsrip/vbp_initiatives/supplemental_programs.htm.
- New York State Department of Health, “DSRIP Project Design Grant (PDG) Payments” (April 2015), www.health.ny.gov/health_care/medicaid/redesign/dsrip/design_grant_payments.htm.
- New York State Department of Health, New York Medicaid Redesign Team (MRT) Waiver Number 11-W-00114/2 (January 19, 2017), p. 56, www.health.ny.gov/health_care/managed_care/appextension/docs/2017-01-19_renewal_stc.pdf.
- New York State Department of Health, “Dashboard B9 Health Home Enrollment” (accessed November 1, 2017), https://dsripdashboards.health.ny.gov/, and Health Homes Implementation Update (May 2013), www.health.ny.gov/health_care/medicaid/program/medicaid_health_homes/docs/2013-05-30_hh_implemt_update.pdf.
- New York State Department of Health, Medicaid Managed Care Enrollment Report – December 2010 (December 2010), p. 8, www.health.ny.gov/health_care/managed_care/reports/enrollment/monthly/2010/docs/en12_10.pdf, and “Number of Medicaid Enrollees by Category of Eligibility by Social Service District - Calendar Year 2010” (May 2011), www.health.ny.gov/statistics/health_care/medicaid/eligible_expenditures/el2010/2010-cy_enrollees.htm.
- Kaiser Family Foundation, “Number of Dual Eligible Beneficiaries” (accessed November 1, 2017), www.kff.org/medicaid/state-indicator/dual-eligible-beneficiaries/?currentTimeframe=0&sortModel=%7B%22colId%22:%22Location%22,%22sort%22:%22asc%22%7D.
- New York State Department of Health, Medicaid Managed Care Enrollment Report – October 2017 (October 2017), p. 19, www.health.ny.gov/health_care/managed_care/reports/enrollment/monthly/2017/docs/en10_17.pdf.
- New York State Department of Health, Medicaid Managed Care Enrollment Report – October 2017 (October 2017), p. 31, www.health.ny.gov/health_care/managed_care/reports/enrollment/monthly/2017/docs/en10_17.pdf.
- New York State Office for People with Developmental Disabilities, “NYS DOH and OPWDD announce a partnership to improve care for individuals with intellectual and developmental disabilities (IDD) who are eligible for both Medicare and Medicaid (‘Medicare-Medicaid Enrollees’)” (accessed November 2, 2017), https://opwdd.ny.gov/news_and_publications/fida-idd-announcement; and Robert Megna, Director, New York State Division of the Budget, “Update on Medicaid Budget” (presentation on January 13, 2011), p. 50, www.health.ny.gov/health_care/medicaid/redesign/docs/2011-01-13_redesign_team_presentation.pdf. The presentation indicates 50,000 people with developmental disabilities account for $6.4 billion in Medicaid spending in an unspecified fiscal year.
- New York State Department of Health, A Path Toward Value Based Payment: Annual Update (June 2016), p. 60, www.health.ny.gov/health_care/medicaid/redesign/dsrip/2017/docs/2016-06_vbp_roadmap_final.pdf.
- DSRIP and other waiver programs are in accordance with the standard terms and conditions negotiated by the New York State Department of Health and the Centers for Medicare and Medicaid Services. See: New York State Department of Health, New York Medicaid Redesign Team (MRT) Waiver Number 11-W-00114/2 (January 19, 2017), www.health.ny.gov/health_care/managed_care/appextension/docs/2017-01-19_renewal_stc.pdf.
- New York State Department of Health, Attachment J – NY DSRIP Strategies Menu and Metrics (accessed November 1, 2017), www.health.ny.gov/health_care/medicaid/redesign/docs/strategies_and_metrics_menu.pdf.
- The PPSs formed cover all counties in New York State, with some counties being served by multiple PPSs. See: New York State Department of Health, “DSRIP Performing Provider Systems (PPS)” (September 2017), www.health.ny.gov/health_care/medicaid/redesign/dsrip/pps_map/index.htm.
- Revenue available to PPSs will be earned based on reporting and performance metrics. Accordingly, PPSs may earn less revenue than is available. Available revenue does not include additional funding which could be earned through small pots of revenue available through “high performance pools.”
- This is a simplified version of the federal requirement that serves as a shorthand summary. The requirement is that 95 percent of the funds go to Medicaid “safety net” providers, with those providers having a more specific definition in terms of their mix of patients. Thus, in addition to some CBOs, some Medicaid providers, such as private physicians who serve relatively few Medicaid patients, would also fall outside the 95 percent limit. See New York Medicaid Redesign Team (MRT) Waiver Number 11-W-00114/2 (January 19, 2017), p. 56, www.health.ny.gov/health_care/managed_care/appextension/docs/2017-01-19_renewal_stc.pdf.
- New York State Department of Health, A Path Toward Value Based Payment: Annual Update (June 2016), p. 42, www.health.ny.gov/health_care/medicaid/redesign/dsrip/2017/docs/2016-06_vbp_roadmap_final.pdf.
- New York State Department of Health, DSRIP Special Terms and Conditions (April 2014), p. 65, www.health.ny.gov/health_care/medicaid/redesign/docs/special_terms_and_conditions.pdf.
- Data for all payments made to individual CBOs is incomplete because not all data is publicly available for three reasons. First, funds flow data from waiver revenues to providers was first included in the fourth quarter of reporting, making all payments in the first three quarters unavailable. Second, funds flow data from non-waiver revenues to providers was first included in the sixth quarter of reporting, making all payments in the first five quarters unavailable. Third, some payments to downstream providers are not made directly by the PPS, but are instead coordinated through CBOs and other downstream providers in the PPS. All available data for payments to individual PPS partners was collected through DSRIP quarterly reports of funds flows, where available. See: New York State Department of Health, PPS Quarterly Reports for Year 2 Quarter 4 (June 30, 2017), Modules 1.3 and 1.9, www.health.ny.gov/health_care/medicaid/redesign/dsrip/quarterly_rpts/.
- Although a medical practice, Brentwood Pediatric and Adolescent Associates was classified by State definition as a CBO; see endnote 16 for a possible explanation.
- See: New York State Department of Health, Request for Applications #1512160408 for Community Based Organization (CBO) Planning Grant (May 2016), www.hinmanstraub.com/newsletter/Community%20Based%20Organizations%20(CBO)%20Planning%20Grant.pdf.
- New York State Department of Health, Office of Health Insurance Programs DSRIP Program, Community Based Organization (CBO) Planning Grant, RFA#1612201231, December 29, 2016, p. 5.
- See: New York State Department of Health, Delivery System Reform Incentive Payment Program (DSRIP) Whiteboard Video- “Best Practices in DSRIP Year 3” – Companion Document (October 2017), www.health.ny.gov/health_care/medicaid/redesign/dsrip/2017/docs/best_pract_dy3.pdf.
- See: New York State Department of Health, Medicaid Redesign Team, “VBP Social Determinants of Health (SDH) & Community Based Organizations (CBOs) Informational Webinar,” August 25, 2017, www.health.ny.gov/health_care/medicaid/redesign/dsrip/vbp_library/docs/2017-08-25_sdh_cbo_slides.pdf.
- This issue is discussed in Deborah Bachrach and others, Implementing New York’s DSRIP Program: Implications for Medicaid Payment and Delivery System Reform (The Commonwealth Fund, April 2016), www.commonwealthfund.org/publications/fund-reports/2016/apr/new-york-dsrip-medicaid.
- Naderah Pourat, California Public Hospitals Improved Quality of Care Under Medicaid Waiver Program, (UCLA Center for Health Policy Research, June 2017), http://healthpolicy.ucla.edu/publications/Documents/PDF/2017/dsrip-brief-jun2017.pdf; and UCLA Center for Health Policy Research, Final Evaluation Report of California’s Delivery System Reform Incentive Payments (DSRIP) Program (February 2016), www.dhcs.ca.gov/provgovpart/Documents/DSRIPFinalEval.pdf.
- Jocelyn Guyer and others, Key Themes from Delivery System Reform Incentive Payment (DSRIP) Waivers in 4 States (Kaiser Commission on Medicaid and the Uninsured, April 2015), p. 5, www.kff.org/medicaid/issue-brief/key-themes-from-delivery-system-reform-incentive-payment-dsrip-waivers-in-4-states/.
- See: Melanie Schoenberg and others, State Experiences Designing and Implementing Medicaid Delivery System Reform Incentive Payment (DSRIP) Pools (National Academy for State Health Policy, March 2015), www.macpac.gov/wp-content/uploads/2015/06/State-Experiences-Designing-DSRIP-Pools.pdf; and Jocelyn Guyer and others, Key Themes from Delivery System Reform Incentive Payment (DSRIP) Waivers in 4 States (Kaiser Commission on Medicaid and the Uninsured, April 2015), www.kff.org/medicaid/issue-brief/key-themes-from-delivery-system-reform-incentive-payment-dsrip-waivers-in-4-states/.
- Massachusetts Executive Office of Health and Human Services, Delivery System Transformation Initiatives Status Report (March 16, 2016), www.mass.gov/eohhs/docs/masshealth/research/legislature-reports/dsti-delivery-system-transformation-initiatives-status-report-03-16-16.pdf.
- Massachusetts Executive Office of Health and Human Services, Attachment M: Massachusetts Delivery System Reform Incentive Payment (DSRIP) Protocol, www.mass.gov/eohhs/docs/eohhs/healthcare-reform/masshealth-innovations/dsrip-protocol.pdf.
- Massachusetts Executive Office of Health and Human Services, MassHealth Behavioral Health Services for Children and Youth Aged 20 and Younger A Guide for Staff Who Work with Children, Youths, and Families (October 2015), p. 31, www.mass.gov/eohhs/docs/masshealth/cbhi/cbhi-guide.pdf.
- Massachusetts Executive Office of Health and Human Services, Attachment M: Massachusetts Delivery System Reform Incentive Payment (DSRIP) Protocol, p. 16, www.mass.gov/eohhs/docs/eohhs/healthcare-reform/masshealth-innovations/dsrip-protocol.pdf.